Carpal Tunnel Syndrome: Symptoms, Diagnosis, Underlying Causes, and Treatment Options
Carpal Tunnel Syndrome is more than just a wrist ache; it is a progressive condition that disrupts sleep, work, and hobbies for millions. If you are experiencing numbness, tingling, or a weakening grip, waiting is not a strategy; it’s a risk.
This guide cuts through the noise to give you a clear, evidence-based roadmap for recovery, whether you are newly diagnosed or trying to avoid unnecessary surgery.


What You Need to Know About Symptoms and Diagnosis
Carpal tunnel syndrome affects millions of people who type, grip tools, drive, sew, or care for children. It presents as tingling, numbness, or pain in the thumb, index, and middle fingers, and can wake you at night or limit your grip strength. Left unaddressed, symptoms can interfere with work, lifting, and hobbies.
This guide provides clear and concise explanations of symptoms, diagnosis, underlying causes, and treatment options. It is for anyone who suspects carpal tunnel syndrome, has a new diagnosis, or wants to avoid unnecessary procedures. You will learn what to do first, what to avoid, and how to measure progress using validated tools.
Definitions and Core Concepts
What is carpal tunnel syndrome?
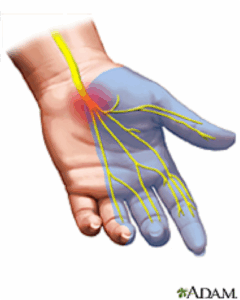
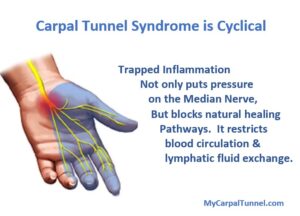
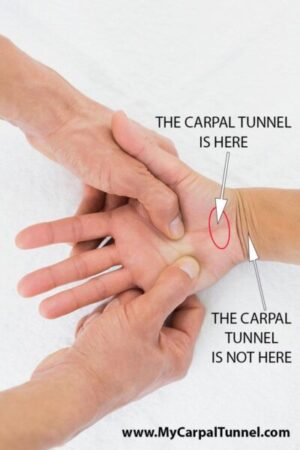
Carpal tunnel syndrome, or CTS, occurs when the median nerve is compressed within the carpal tunnel, a narrow passageway in the wrist. Swelling of the tendon sheaths, fluid retention, or structural crowding increases pressure, which impairs nerve function and produces sensory symptoms, as well as sometimes weakness in the thumb muscles.
Why do symptoms occur?
The median nerve supplies sensation to the thumb, index, middle, and part of the ring finger, and motor fibers to the thenar muscles. Compression causes paresthesia, pain, clumsiness, and nocturnal awakening. Common contributors include repetitive wrist activities, pregnancy, diabetes, hypothyroidism, obesity, and inflammatory arthritis, which can increase tunnel pressure or tissue volume.
Step-by-Step: How to Get a Confident Diagnosis and Relief

- Recognize classic symptoms
Expect numbness or tingling in the thumb, index finger, and middle finger, which is typically worse at night or with sustained wrist flexion or gripping. Hand clumsiness, dropping objects, and pain radiating up the forearm are common. Constant numbness or thenar atrophy suggests more severe compression. - Try simple provocative tests at home, then seek a clinical exam.
Flexing the wrist for 60 seconds (Phalen test), tapping over the carpal tunnel (Tinel test), or applying direct compression (Durkan test) can reproduce symptoms. These tests vary in accuracy, so a clinician should interpret the results alongside your medical history. Recent analyses report moderate sensitivity and specificity for these maneuvers, which means they guide but do not confirm the diagnosis. - Get appropriate confirmatory testing when needed.
Electrodiagnostic studies, specifically nerve conduction studies with or without electromyography, remain the standard for confirming median neuropathy, grading its severity, and ruling out mimics such as radiculopathy or ulnar neuropathy. Neuromuscular ultrasound can visualize median nerve swelling and has diagnostic accuracy similar to electrodiagnostic testing in many settings, helping to identify structural causes, such as ganglion cysts. - Start with low-risk measures.
Modify provoking tasks, optimize ergonomics, and consider a neutral wrist night splint trial for a few weeks. Evidence for splints is mixed, but some people report overall improvement, especially when symptoms are mild and recent. Avoid prolonged daytime immobilization, as this can worsen stiffness. - Address contributing conditions.
Manage diabetes, thyroid disease, and inflammatory arthritis in collaboration with your clinician. Pregnancy-related CTS often improves postpartum, so conservative care is preferred unless severe deficits emerge. - Consider targeted treatments for persistent symptoms.
Local corticosteroid injection provides short-term relief and can reduce the need for surgery in some cases, with effects lasting up to 12 months. Expect benefits for up to six months on average in mild to moderate CTS, with serious adverse events rare in trials. If symptoms recur, discuss the timing and alternatives with your healthcare provider. - Escalate to surgery when indicated.
Surgery (open or endoscopic carpal tunnel release) is appropriate for severe, progressive, or refractory symptoms, especially with constant numbness, weakness, or marked electrodiagnostic abnormalities. Most studies report good outcomes for appropriately selected patients, though recurrence definitions vary widely across research.
Pitfalls to avoid: Do not ignore progressive weakness or constant numbness. Do not rely solely on pain pills. Do not assume splinting alone will fix long-standing, severe disease.
Strategies and Frameworks That Work
The “RELIEF” Framework for CTS
-
- R, Recognize early symptoms and triggers, including night numbness and device or tool positions that flex the wrist. This proactive approach can help you take control of your condition and seek timely medical advice.
-
- E, Examine with clinician-guided tests and confirm with electrodiagnostic studies or ultrasound if needed. Remember, you’re not alone in this journey. Your clinician is there to guide you every step of the way.
-
- L, Limiting aggravating loads, improving ergonomics, and using a neutral wrist at night for a defined trial are essential strategies. These measures can help you manage your condition effectively.
-
- I, Inject judiciously for short-to-intermediate relief in mild to moderate cases or to bridge to definitive decisions.
-
- E, Escalate to surgery for severe or refractory disease based on symptoms, function, and objective severity.
-
- F, Follow outcomes using a validated patient-reported scale like the Boston Carpal Tunnel Questionnaire to quantify progress.
When to choose each path
-
- Conservative-first: Mild, intermittent nocturnal symptoms without weakness, short symptom duration, or pregnancy.
-
- Injection as a bridge: Persistent symptoms that limit sleep or work after splinting and activity changes, but without thenar atrophy or constant numbness.
-
- Surgery: Thenar weakness, constant sensory loss, severe electrodiagnostic abnormalities, or failure of conservative measures.
Tools and Options: Comparison Table
| Option | Best For | Key Features | Limitations |
| Education and ergonomics | Mild, early CTS; work-related triggers | Neutral wrist positions, rest breaks, task rotation | Requires behavior change; benefits build over weeks |
| Night wrist splint (neutral) | Nocturnal paresthesias; short-duration symptoms | Low cost, easy to try | Mixed evidence on symptoms and function; avoid prolonged daytime immobilization |
| Local corticosteroid injection | Mild to moderate CTS needing quick relief | Relief up to six months; may delay surgery up to 12 months | Relief is usually temporary; consider risks with repeated injections |
| Oral analgesics (short-term) | Short-term pain relief | May ease pain to sleep or function | Do not address nerve compression; NSAID evidence is limited or inferior to injection in trials |
| Physical therapy modalities | Select cases, especially posture or strength deficits | Nerve-gliding, proximal strengthening, and education | Evidence quality varies; it must be individualized |
| Ultrasound-guided interventions | Selected cases with clear structural targets | Precise targeting, diagnostic insights | Requires expertise and access |
| Surgery (open or endoscopic release) | Severe, progressive, or refractory CTS | Frees the nerve, high rates of symptom improvement | Recovery time, rare complications; recurrence definitions vary across studies |
Common Mistakes and How to Fix Them
- Waiting too long with progressive weakness: If you notice thumb weakness or persistent numbness, consult a specialist. Objective deficits raise the urgency for surgery.
- Using splints around the clock: Night use is reasonable, but full-time immobilization can stiffen joints without adding benefit. Limit daytime use unless you need to protect your wrist during heavy tasks.
- Relying on pain pills alone: Analgesics do not decompress the nerve and should not be the core strategy. Use them sparingly and focus on mechanical and targeted treatments.
- Skipping confirmatory testing in atypical cases: Electrodiagnostic studies and ultrasound can help clarify the diagnosis and severity, as well as rule out mimics, leading to more informed decisions.
- Assuming all numb hands are CTS: Cervical radiculopathy, ulnar neuropathy, and systemic neuropathies can mimic CTS. Proper evaluation prevents misdirected treatment.
Measurement and KPIs: Track Your Progress
Use validated patient-reported measures.
The Boston Carpal Tunnel Questionnaire (BCTQ) is a reliable, valid, and responsive measure, making it a practical primary outcome measure. It includes a Symptom Severity Scale and a Functional Status Scale, each scored 1 to 5, where higher scores indicate worse outcomes.
Simple tracking plan:
- Baseline: Record BCTQ scores, night awakenings per week, and grip pinch tasks that fail.
- After 2–4 weeks of conservative care, expect to see slight reductions in nocturnal symptoms and improved task tolerance if the plan is effective.
- After injection: Expect marked symptom reduction within 1–2 weeks, often lasting weeks to months, with reassessment at 6–12 weeks.
- After surgery: Expect progressive improvement in paresthesias and function over months. Many series report 75 to 90 percent clinical success, though definitions differ, and some patients note recurrent or residual symptoms.
Basic formulas and thresholds:
- BCTQ improvement: Aim for at least a 0.5 to 1.0 point reduction on the 1–5 scale as clinically meaningful over 6–12 weeks.
- Night awakening count: Reduce awakenings by 50 percent within one month of starting a splint or injection plan.
- Function anchors: Track opening jars, type for 30 minutes without experiencing numbness, and maintain uninterrupted sleep stretches.
Real-World Mini Case Study: From Night Numbness to Normal Workdays
Profile:
Alex, a 42-year-old graphic designer, reports three months of nighttime hand numbness, worse after long editing sessions. She drops her phone on occasion and wakes up twice nightly.
Evaluation:
Symptoms localize to the thumb, index, and middle fingers. Phalen’s test reproduces tingling within 30 seconds. No thenar atrophy is noted. The clinician reviews workstation photos that show wrist flexion on a low keyboard tray.
Plan:
Alex starts with education and ergonomics, moves to a neutral wrist night splint, and adopts microbreaks. After three weeks, night awakenings fall from two to one but persist. A local corticosteroid injection is offered and performed. She continues with ergonomics and splinting for two more weeks.
Outcome:
At six weeks, Alex’s BCTQ Symptom score drops from 3.0 to 1.6. She sleeps through most nights and works without frequent numbness. The plan is to maintain ergonomics and reevaluate if symptoms recur, with surgery reserved for worsening weakness or return of constant numbness.
Key Takeaways
- CTS is a median nerve compression that produces numbness, tingling, and weakness, often worse at night.
- A confident diagnosis combines symptom pattern, exam maneuvers, and targeted confirmatory testing when needed.
- Start with low-risk measures, such as ergonomic adjustments and a time-limited night splint trial, and then consider injection therapy for persistent symptoms.
- Surgery is effective for appropriately selected patients, especially with progressive weakness or refractory symptoms.
- Track progress with validated tools like the BCTQ and objective functional anchors.